SPECIAL REPORT: Breaking Down the UK Flu Scare Coming to America
A data-driven analysis of the current flu season from the UK to the U.S.

Surge…Racing towards records…Worst case scenario – these are the words deliberately chosen by the UK’s corporate media over the last weeks when reporting on the flu coming into the holiday season.
Ignoring all the lessons from the failed pandemic response, the UK and it’s compliant media didn’t miss a beat reflexively calling for masking, lockdowns and activity closing schools.
Are we entering a flu epidemic? And is America next in line? New Variant Raises Concerns of Another Bad Flu Season writes The NY Times. CDC officials urge US flu vaccination writes The Guardian.
Lets attack this narrative at its core starting with UK data. It’s important to note first that around 1998, the UK lowered its threshold for calling a pandemic. Shown in the graph below, from 1988 to 1998 an epidemic of influenza-like-illness (ILI) was 400 weekly consultations (visits to primary care doctors) per 100,000. After that date, it was lowered to 200 or above.

With that in mind, lets look at the current UK and England data from their own government monitoring.
Currently the weekly general practitioner consultation rate of ILI in England is 18.3 per 100,000. Not an epidemic as the media hype would lead viewers to believe.

In fact, the UK’s own report of official statistics states as its main message of the entire report the following:
“Influenza activity increased and is circulating at medium levels”
ILI is a catch-all term. It could be anything – COVID, RSV, flu, a head cold of unknown origin. So to get more focused data, we head to the UK’s Respiratory DataMart – the sentinel laboratory-based surveillance system where participating laboratories report positive and negative test results for a number of respiratory viruses from samples primarily taken in hospital.
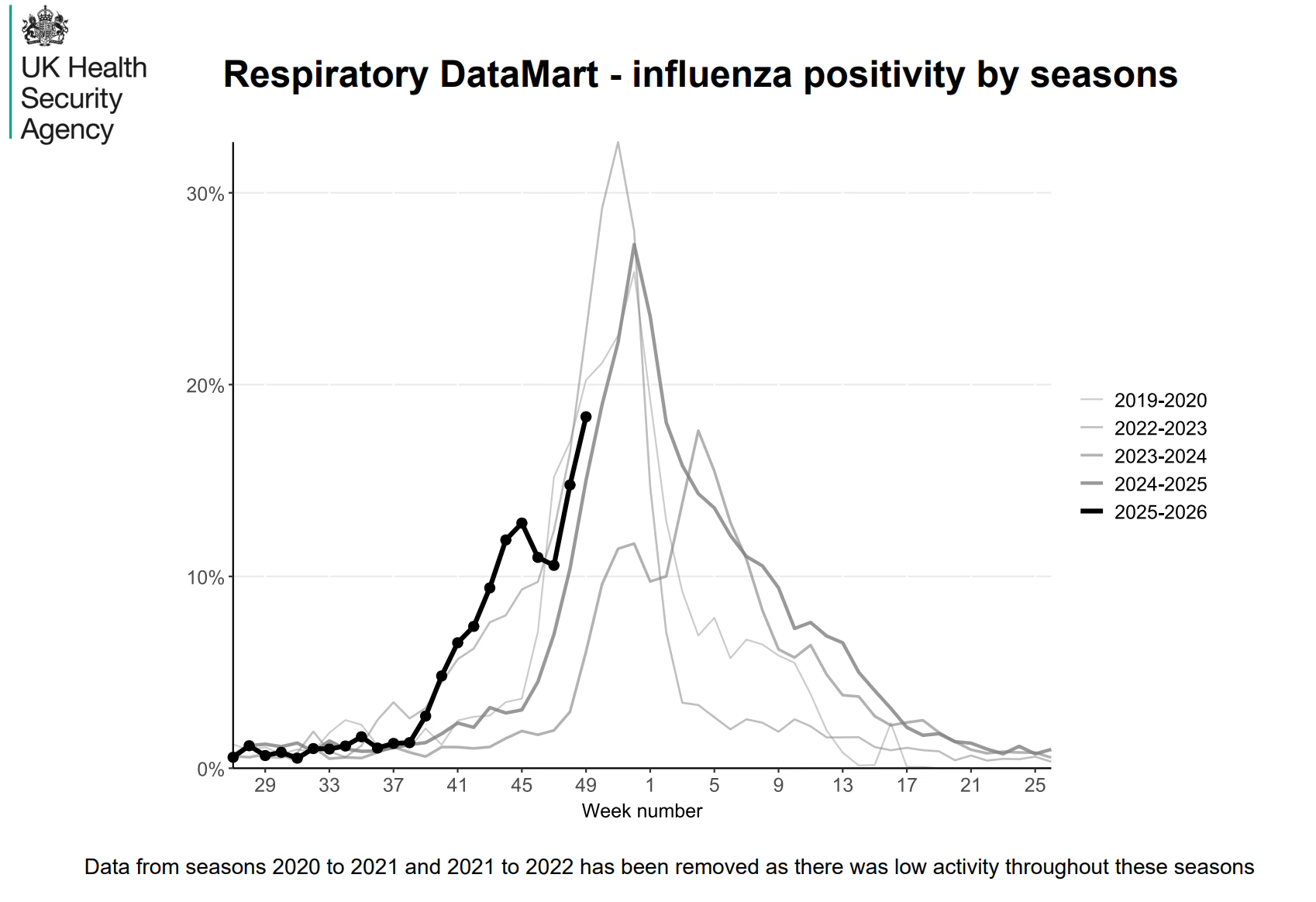
As the graph shows, an unremarkable, average uptrend as the normal flu season ramps up – much like it always does as shown in the gray lines from previous years.
Alongside fear narrative coverage to scare the public, parallel stories of an overwhelmed NHS hospital system are being reported. According to the UK.gov data, hospital ICU admission rates for ILI remain low by their own ranking system.

So why is a normal flu season overwhelming the NHS healthcare system?
According to the British Medical Association (BMA), there is a major, institutional deficit of practicing doctors in England and the UK. Literally, as soon as one becomes a doctor, they are by definition, overwhelmed.
Is a flu virus causing this?
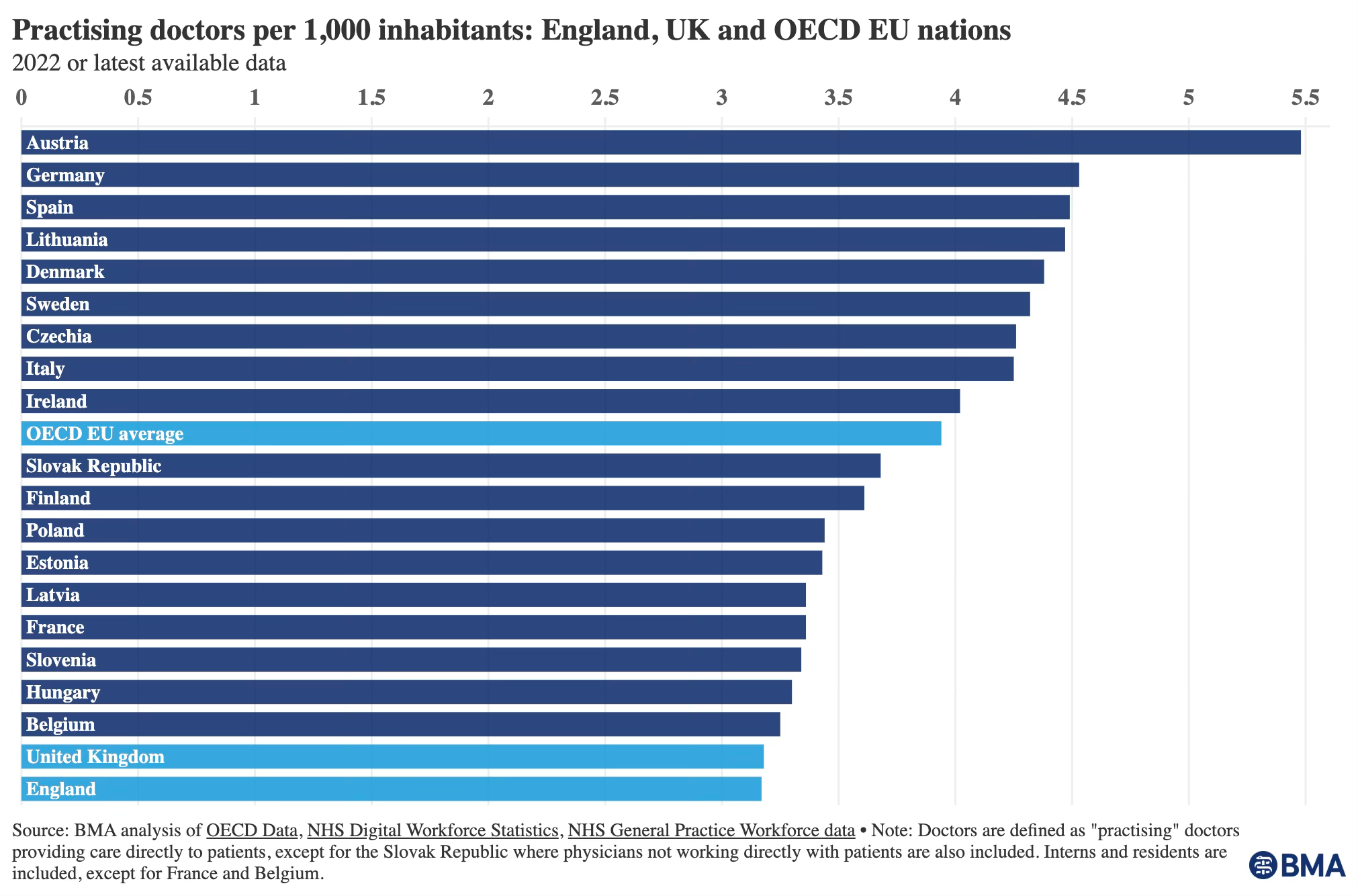
According to the latest BMA report:
“The NHS has a chronic workforce crisis, driven by years of inadequate workforce planning, lack of accountability for workforce issues and recurrent failure to value and invest in staff. Without action to better train and retain the doctors the NHS needs, staffing levels WILL continue to fall short of demand, further impacting working conditions, waiting lists and care quality.”
NHS healthcare staff have been engaged in negotiations for better pay and working conditions. Around the same time the government rejected their demands, the media whipped up a flu scare narrative amounting to essentially a public blackmailing of NHS staff to not strike during a ‘flu surge.’
BBC news ran the headline: Doctor strike during flu outbreak would be ‘reckless’, says UK PM Keir Starmer
Meanwhile, the BMA activated and sided with its medical professionals with its latest press release.

The BMA wrote:
“It is horrible for anyone to be suffering with flu – we are not diminishing the impact of that – but Mr Streeting should not be scaremongering the public into thinking that the NHS will not be able to look after them and their loved ones.
Now onto the United States corporate media reporting, who at this stage, are beginning to build on the UK fear narrative with headlines like the following:
Experts worry the U.S. is in for another bad flu season -NPR
Terrifying maps show exactly who is at risk of new ‘super flu’ in US - Daily Mail
Looking at the CDC’s flu and ILI monitoring networks, there are currently 547 influenza positive test reports registered to the CDC – down from the previous 3 weeks.
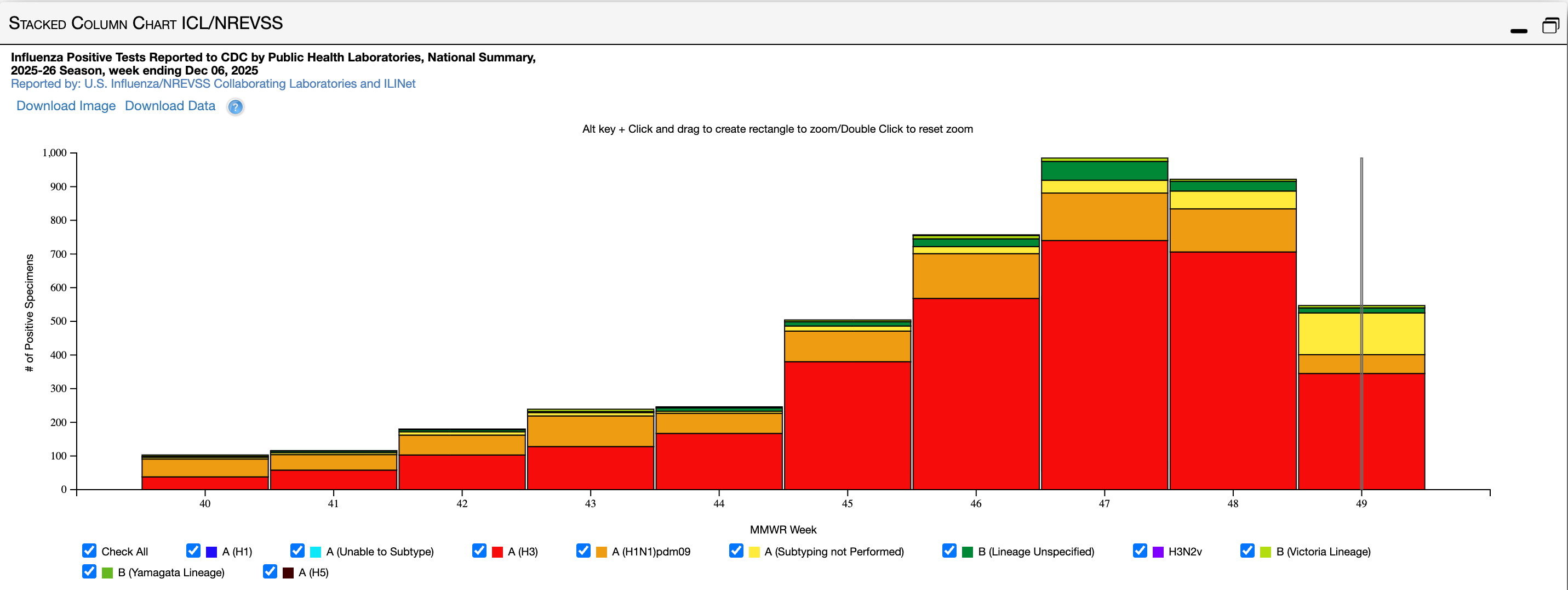
At the same time last year there were 1,632. The year before that 2,803.
Lets talk about the flu shot being pushed as the only solution to this year’s so far average flu season.
In an internal memo leaked to the media, FDA head at the Center for Biologics Evaluation and Research Vinay Prasad stated as a goal:
We will revise the annual flu vaccine framework, which is an evidence-based catastrophe of low quality evidence, poor surrogate assays, and uncertain vaccine effectiveness measured in case-control studies with poor methods. We will reappraise safety and be honest in vaccine labels.
The regulatory framework for the flu shot is a mess. And the public should be demanding better data and accountability before being roped into accepting a another year of a product with poorly defined safety and efficacy.
Each year, the flu vaccine is developed by global surveillance tracking circulating viruses, predicting (guessing) dominant strains, selecting them in February (Northern Hemisphere), and then mass-producing vaccines using methods like growing viruses in chicken eggs (traditional), animal cells.
This year, they guessed wrong.
The new influenza A(H3N2) virus strain renamed “H3N2 subclade K,” was identified by health organizations months after the seasonal influenza vaccine was developed.
According to the CDC, they currently do not have the data to report on vaccine effectiveness for the annual shot chosen this year:
Influenza vaccine effectiveness networks are collecting real-world data to produce early estimates of influenza vaccine effectiveness in the United States once influenza activity has increased and sufficient data have been collected to conduct these analyses.
No data on an annual flu shot that omitted the dominate strain circulating this year embedded within a wider framework called an “evidence-based catastrophe of low quality evidence, poor surrogate assays.”